*僅供醫學專業人士閱讀參考
甲銀屑病有何新進展?EADV2022為您帶來精彩介紹
?
銀屑病是遺傳因素和環境因素(感染、外傷、藥物)等多種因素相互作用的多基因遺傳病,是經過免疫介導的共同通路最后引起角質形成細胞發生增殖。臨床上分為尋常型,紅皮病型,關節病型和膿皰型。銀屑病除了皮膚、關節、黏膜受累外,還會累及到指(趾)甲(稱為甲銀屑病)。隨著甲的逐步損害,也會對患者的工作、學習、生活和社交等產生非常大的影響。那么2022年關于甲銀屑病有什么新進展呢?在今年的歐洲皮膚病與性病學會年會(EADV)上,來自布魯格曼大學醫院的Bertrand RICHERT博士分享了題為《NAIL PSORIASIS best management and newinsights》(甲銀屑病:最佳的管理方法和新的見解)的相關內容。“醫學界”舉辦了一場國內專家解讀國際會議的活動——“皮膚青委帶你看EADV 2022”,有幸邀請到來自上海交通大學醫學院附屬瑞金醫院皮膚科主任醫師曹華教授進行解讀,一起看下去吧!
1
甲銀屑病的臨床特征了解甲銀屑病的臨床特征對于治療很關鍵。甲銀屑病的臨床特征取決于炎癥侵蝕的部位,分為兩大類。一類是甲基質損害,甲基質損害有兩種表現,一種是頂針樣外觀,另一種是近端白甲,與甲真菌病非常相似。
一類是甲床損害。甲床受累在患者中的發病率更高,有油滴樣改變、甲剝離和甲下角化過度。
患者可能有甲基質損害,或甲床損害,或兩種損害同時存在。
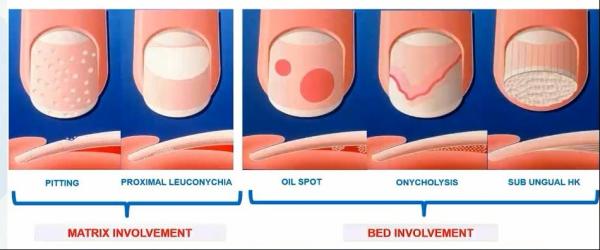
圖1 指甲型銀屑病的臨床特征
2012年Love TJ等人[1]的研究中就提出,與其他臨床表現相比,指甲剝離與銀屑病關節炎(psoriatic arthritis,PsA) 更相關。相關研究數據還顯示,所有的銀屑病患者中,有近80%的患者存在指甲受累。其中PsA中甲銀屑病的發病率最高,能達到90%以上。因此在臨床中碰到患者有指甲損害時是否還同時存在關節受累,也許早期PsA的診斷率也會提高。

圖2 甲剝離與PsA 風險相關[1]
2
甲銀屑病的診斷要點
有研究[2]指出,皮膚嚴重程度、指甲嚴重程度和PsA風險之間沒有相關性。而PsA風險與指甲受累的時間相同[3,4]。還有研究[5]指出,84%的患者在關節疾病發生前約有12年的皮膚和指甲受累。而不符合CASPAR的患者存在關節受累的亞臨床證據[6],比如影像學的改變,有些患者早期無關節疼痛或腫脹,并且在X影像中是看不到關節受累,但是高分辨率MRI中提示附著點炎或骨炎,這就是經典的亞臨床改變。因此對于這樣的患者要加強早期診斷和隨訪。
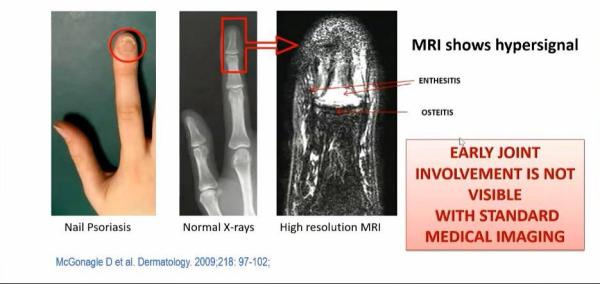
圖3 早期MRI影像學表現[7]
患者關節附著點炎或骨炎的超聲信號是增強的,存在甲下組織增厚,伸肌腱附著點增厚[8]。因此認為MRI和超聲可以發現早期炎癥改變[9,10],但MRI是診斷的金標準[11]。
?

圖4 早期超聲表現[7]
與沒有甲受累的患者相比,甲銀屑病患者需要更多的時間達到PASI 75,提示有甲損害的患者預后較差。由于皮膚的生長周期不同,所以與甲損害相比,皮損對生物制劑有更好的應答。
3
甲銀屑病的治療選擇銀屑病的治療仍面臨很大挑戰1、治療方法有限,不能在短期內看到好的效果。2、由于短期療效不明顯,因此患者治療依從性差,不能持續治療,導致治療不完全。3、容易復發。4、此外還有其他因素影響治療效果,比如指甲的病變部位、皮膚有無受累、關節有無受累、職業、社會和心理影響、是否伴有合并癥等。
目前甲銀屑病的治療主要包括局部治療和系統治療等兩種方法。Bertrand RICHERT博士指出局部外用藥物較難使藥物滲透到甲床和甲基質,局部使用糖皮質激素、他扎羅汀、Vit D類似物或卡泊三醇聯合倍他米松外用治療的療效無顯著差異。當發生甲剝離時,需要修剪所有脫落的指甲,使藥物與病甲充分接觸,和甲真菌病的治療很相似。Bertrand RICHERT博士在臨床中曾采用修剪病甲聯合卡泊三醇和倍他米松的方案治療6個月或者單用二丙酸氯倍他索治療6個月,獲得較為滿意的效果。所以要和患者做好解釋工作,用藥有效,但是治療時間較久,提高患者依從性。


圖5 修剪病甲聯合卡泊三醇+倍他米松(6個月)

圖6 二丙酸氯倍他索(6個月)
 圖7 曲安奈德局部病灶內注射用藥[12]
圖7 曲安奈德局部病灶內注射用藥[12]此外還有一個病例報道[13]講述了在病灶內注射甲氨蝶呤成功治療1例甲型銀屑病,該患者使用濃度為2.5mg/ml的甲氨蝶呤,每個指甲基質內0.1ml(= 2.5mg/10指),1個月1次,治療持續3個月,也獲得非常好的療效。此后還有多項類似報道[14,15]。
?
 圖8 甲氨蝶呤局部病灶內注射用藥[13]
圖8 甲氨蝶呤局部病灶內注射用藥[13]
有文獻[16]中詳細介紹了甲氨蝶呤的注射方法,先在指甲兩側的間隙內注射0.5ml利多卡因(2%)進行環形阻滯,然后在指甲交界處2.5 mm的位置向指甲兩側注射2.5 mg甲氨蝶呤。國外還有不少類似的研究報道,但日后還需要更多研究來確定最佳注射濃度和注射頻率。

圖9 甲氨蝶呤注射方法[16]


2、第二種方法:使用阿維A進行系統治療[20,21],小劑量阿維A0.2-0.3 mg/kg/d在治療6個月時NAPSI可以下降40.9%,這種治療方法對甲床角化過度最有效。
3、第三種方法:使用環孢素治療。環孢素治療是作為推薦寫入歐美國家的指南中,法國指南中提出第一推薦甲氨蝶呤,第二推薦環孢素或二代維甲酸。使用環孢素3-5mg/kg/d,分2次口服,甲床受累患者的療效要優于基質受累的患者。環孢素雖然對皮損控制較快,但是停藥或減藥后復發也較快。對于有生育要求的患者也不建議使用環孢素[18,19]。
另一項研究[22]納入了84例患者,進行了3年的回顧,患者分別使用了阿維A、MTX、CyA、PUVA、rePUVA、NUVB、ReNUVB +所有生物制劑,NaPSI評分的平均基線為14.7分,58%的患者采用經典的系統治療,其中生物制劑占42%。結果發現24周時藥物的療效一致,但環孢素起效最快。
?

圖12 NAPSI評分演變與系統治療方法比較[22]
一項開放性標簽研究[23]發現阿普斯特可以改善甲銀屑病患者的指甲病變,這項研究納入了11名患者,沒有設置安慰劑組,使用阿普斯特30mg,日2次口服,共治療?52周,其中在第8周就獲得很好地療效,52周指甲基本恢復正常。療效評價提示,大部分患者從12周開始mNAPSI評分與基線水平相比都有顯著差異。
?

有研究[24]表明,在甲銀屑病的治療中引入生物制劑和小分子藥物可以快速控制疾病并提高療效。在ESTEEM研究中使用阿普斯特30mg/天治療,結果發現在第16周時NaPSI降低22% ~ 29%,第32周時NaPSI降低43- 60%,第52周時NaPSI降低60%。在APPRECIATE研究中納入250名患者,結果發現患者和醫生滿意度評分均有較好的改善[25]。
因此認為甲銀屑病是較難治療的部位。治療反應慢于皮膚銀屑病,一般在6個月以上進行評估,療效的評估排序是困難的,存在一定偏倚+ + +。多項研究[26-29]比較發現,生物制劑治療尚未顯示任何優勢。
一項薈萃分析[30]比較生物制劑對銀屑病甲完全緩解的療效,結果發現在中度至重度銀屑病合并銀屑病甲損害的患者中,依奇珠單抗在批準的生物制劑中最有可能在第 24-26 周實現銀屑病甲損害的完全消退。如果銀屑病甲損害合并有PsA時應首選TNF-α抗體或IL-17抗體治療。
?

圖14 生物制劑對銀屑病甲完全緩解的療效比較[30]
此外有一項研究[31]發現小分子藥物JAK 1/3抑制劑托法替布在治療甲銀屑病也有很好的療效,有研究結果發現,與安慰劑相比,托法替尼治療16周時甲銀屑病的病情有所改善,持續了52周。但是此后還沒有類似的相關研究。
?

圖15 托法替尼治療甲銀屑病的療效比較[31]
3.?治療方案選擇
2、累及>3個指甲時采用局部治療+系統性治療,可以使用阿維A 0.2-0.4mg/天、MTX 15mg/周、環孢素 3.5mg/kg/天或生物制劑(按醫保報銷標準)。
 圖16 指甲型銀屑病的臨床治療方法選擇[32]
圖16 指甲型銀屑病的臨床治療方法選擇[32]
4
總結
1、指甲型銀屑病的治療過程是漫長的,應個體化治療,并做好患者的心理疏導工作。
2、目前仍有許多潛在的治療方法需要臨床醫生去摸索,而且皮膚科醫生可以和風濕病學專家一起合作進行診治。
3、需要早期的醫學成像進行輔助診斷,如超聲和MRI。
4、目前研究發現所有局部用藥和生物制劑的療效都一樣。
5、如果存在甲剝離應早期進行PsA 的評估,盡快使用生物制劑以預防關節破壞。
6、避免同形現象:保護甲單元。
專家簡介

曹華?教授
醫學博士,主任醫師,博士生導師- 現任上海交通大學醫學院附屬瑞金醫院皮膚科副主任
- 兼任中華醫學會皮膚性病學分會青年委員會副主任委員,上海市醫學會皮膚科專科委員會委員,上海醫師協會皮膚性病學分會委員,《英國皮膚科學雜志中文版》、《診斷學理論與實踐》編委。
- 1999年畢業于上海第二醫科大學(上海交通大學醫學院前身),2006年11月至2008年11月在美國康奈爾大學醫學院、美國史隆-凱特林腫瘤研究中心進修免疫學。
- 師從鄭捷教授,擅長紅斑狼瘡、硬皮病、白塞病、皮肌炎、干燥綜合癥、血管炎等自身免疫病和免疫靶向藥物相關性皮膚病的診斷與治療。
- 主持國家自然科學基金4項、上海市自然科學基金和上海市科委醫學引導類等課題。獲得“2017上海交通大學醫學院高峰學科——臨床醫學研究型醫師”。“2019年度上海醫苑新星——杰出青年人才培養計劃”。
- 以第一作者和通訊作者論著發表于Clinical Rheumatology、Arthritis & Care Research、PLoS ONE、Journal of Rheumatology、British Journal of Dermatology、Lupus、Rheumatology、Journal of American Academy of Dermatology等雜志。
參考文獻:
[1]Love?TJ,??Gudjonsson?JE,??Valdimarsson?H,?et al. Psoriatic arthritis and onycholysis results from the cross-sectional Reykjavik psoriatic arthritis study. J Rheumatol?2012 Jul;39(7).[2]Jones SM, Armas JB, Cohen MG, et al. Psoriatic arthritis: outcome of disease subsets and relationship of joint disease to nail and skin disease. ?Br J Rheumatol. 1994;33:834-9.[3]Williamson L, Dalbeth N, Dockerty JL, et al, Wordsworth BP. Extended report: nail disease in psoriatic arthritis--clinically important,potentially treatable and often overlooked. Rheumatology (Oxford). 2004;43:790-4.[4]Scarpa R, Manguso F, Oriente A, Peluso R et al. Is the involvement of the distal interphalangeal joint in psoriatic patients related to nail psoriasis? Clin Rheumatol. 2004;23:27-30.[5]Fitzgerald O, Winchester R. Psoriatic arthritis: from pathogenesis to therapy.Arthritis Res Ther. 2009:11(1):214.[6]Gottlieb AB, Kircik L, Eisen D et al. Use of etanercept for psoriatic arthritis in the dermatology clinic: the Experience Diagnosing, Understanding Care, and Treatment with Etanercept (EDUCATE) study. J Dermatolog Treat. 2006;17(6):343-52.[7]McGonagle D, ?Tan AL, ?Benjamin M,?et al. The nail as a musculoskeletal appendage--implications for an improved understanding of the link between psoriasis and arthritis. Dermatology 2009;218(2).[8]McGonagle D, Tan AL, Benjamin M. Dermatology. 2009;218:97-102.Tan A et al. Rheumatology (Oxford). 2007:46:253-6.[9]Wiell C, Szkudlarek M, Hasselquist M et al. ?Ultrasonography, magnetic resonance imaging,radiography, and clinical assessment of inflammatory and destructive changes in fingers and toes of patients with psoriatic arthritis. Arthritis ResTher.2007;9(6):R119.[10]Bagel J, Schwartzman S. Enthesitis and Dactylitis in Psoriatic Disease: A Guide for Dermatologists. ?Am J Clin Dermatol.2018 Aug 16. ?doi: 10.1007/s40257-018-0377-2.[11]Zabotti A, Mandl P, Zampogna G, Dejaco C, lagnocco A. One year in review 2018: ultrasonography in rheumatoid arthritis and psoriatic arthritis. ?Clin Exp Rheumatol. 2018 ;36(4):519-525.[12]de Berker DA, Lawrence CM. A simplified protocol of steroid injection for psoriatic nail dystrophy. Br J Dermatol.1998;138(1):90-5.[13]Mokni S, Ameur K, Ghariani N, Sriha B, Belajouza C, Denguezli M, Nouira R. A Case of Nail Psoriasis Successfully Treated with Intralesional Methotrexate. Dermatol Ther (Heidelb). 2018 Dec;8(4):647-651.[14]Mittal J, Mahajan BB. Intramatricial injections for nail psoriasis: An open-label comparative study of triamcinolone, methotrexate, and cyclosporine. Indian J Dermatol Venereol Leprol. 2018 Jul-Aug:84(4):419-423.[15]Saricaoglu H, Oz A, Turan H. Nail psoriasis successfully treated with intralesional methotrexate: case report. Dermatology. 2011 Feb;222(1):5-7.[16]Choudhary P, Mehta RD, Ghiya BC, Sharma D. Treatment of nail psoriasis with intramatrical methotrexate: Anuncontrolled prospective study of 20 patients. J Am Acad Dermatol. 2021:84:526-528.[17]Duarte AA, Carneiro GP, Murari CM, Jesus LCB. Nail psoriasis treated with intralesional methotrexate infiltration. An Bras Dermatol. 2019;94:491-492.[18]Amatore F, ?Villani AP, ?Tauber M, et al. French guidelines on the use of systemic treatments for moderate-to-severe psoriasis in adults. ?J Eur Acad Dermatol Venereol 2019 Mar;33(3).[19]Warren RB, ?Mrowietz U, ?von Kiedrowski R, et al. An intensified dosing schedule of subcutaneous methotrexate in patients with moderate to severe plaque-type psoriasis (METOP): a 52 week, multicentre, randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 2017 02 04;389(10068) .[20]Tosti A, Ricotti C, Romanelli P, Cameli N, Piraccini BM. Evaluation of the efficacy of acitretin therapy for nail psoriasis. Arch Dermatol 2009; 145:269-271.[21]Ricceri F, Pescitelli L, Tripo L, Bassi A, Prignano F. Treatment of severe nail psoriasis with acitretin: an impressive therapeutic result. Dermatol Ther. 2013;26:77-8.[22]Sanchez-Regana M, Sola-Ortigosa J, Alsina-Gibert M et al. Nail psoriasis: a retrospective study on the effectiveness of systemic treatments(classical and biological therapy) JEADV 2011;25:579-586.[23]Oak ASW, ?Ho-Pham H, ?Elewski BE,?Improvement of 11 patients with nail psoriasis with apremilast: Results of an investigator-initiated open-label study. J Am Acad Dermatol 2020 Dec;83(6).[24]Rigopoulos D, Stathopoulou A, Gregoriou S. Small Molecules and Biologics in the Treatment of Nail Psoriasis. SkinAppendage Disord. 2020;6:134-141.[25]Augustin M, Radtke M, Schneider J, Pinter A, Wilsmann Theis D, Peter RU, et al. Real- world experience with apremilast: analysis of 250 patients from the APPRECIATE study with psoriasis in difficult-to-treat areas. Pre- sented at the 2019 AAD Annual Meeting; 2019 March 1-5. Washington, DC; 2019.[26]Saraceno R, Pietroleonardo L, Mazzotta A, Zangrilli A, Bianchi L, Chimenti S. TNF-a antagonists and nail psoriasis: an open, 24-week, prospective cohort study in adult patients with psoriasis.?Expert Opin BiolTher. 2013;13:469-73.[27]Kyriakou A, Patsatsi A, Sotiriadis D. Anti-TNF agents and nail psoriasis: a single-center, retrospective, comparative study. J Dermatolog Treat. 2013;24:162-8.[28]?Bardazzi F, Antonucci VA, Tengattini V, Odorici G, Balestri R, Patrizi A. A 36-week retrospective open trial comparing the efficacy of biological therapies in nail psoriasis. ?J Dtsch Dermatol Ges. 2013;11:1065-70.[29]Sanchez-Regana M, Sola-Ortigosa J, Alsina-Gibert M et al. ?Nail psoriasis: a retrospective study on the effectiveness of systemic treatments (classical and biological therapy) JEADV 2011;25:579-586.[30]Reich K, Conrad C, Kristensen L. et al. Network meta-analysis comparing the efficacy of biologic treatments for achieving complete resolution of nail psoriasis. J Dermatolog Treat. 2021 Mar 1:1-9.[31]Merola JF, ?Elewski B, ?Tatulych S, et al. Efficacy of tofacitinib for the treatment of nail psoriasis: Two 52-week, randomized, controlled phase 3 studies in patients with moderate-to-severe plaque psoriasis. J Am Acad Dermatol 2017 Jul;77(1)》[32]?Rigopoulos D, ?Baran R, ?Chiheb S, et al. Recommendations for the definition, evaluation, and treatment of nail psoriasis in adult patients with no or mild skin psoriasis: A dermatologist and nail expert group consensus. J Am Acad Dermatol 2019 Jul;81(1).[33]Megna M, ?Gisonni P, ?Napolitano M, et al. The effect of smartphone addiction on hand joints in psoriatic patients: an ultrasound-based study. J Eur Acad Dermatol Venereol 2018 Jan;32(1).責任編輯:香菜
更多皮膚科臨床知識,哪里學?
你想看的,醫生站App都有??

下載醫生站App,隨時隨地訂閱啦~
版權申明
本文原創,歡迎轉發朋友圈- End -
 醫學界力求其發表內容在審核通過時的準確可靠,但并不對已發表內容的適時性,以及所引用資料(如有)的準確性和完整性等作出任何承諾和保證,亦不承擔因該些內容已過時、所引用資料可能的不準確或不完整等情況引起的任何責任。請相關各方在采用或者以此作為決策依據時另行核查。
醫學界力求其發表內容在審核通過時的準確可靠,但并不對已發表內容的適時性,以及所引用資料(如有)的準確性和完整性等作出任何承諾和保證,亦不承擔因該些內容已過時、所引用資料可能的不準確或不完整等情況引起的任何責任。請相關各方在采用或者以此作為決策依據時另行核查。